Given these changes from the original case, what is your diagnosis?
What is your diagnostic explanation?
As compared to the long case, this patient is a 75 year old male presenting to the ER with reports of headache over the past few weeks. The patient has difficulty focusing during the interview. He is accompanied by his wife, who confirms that he has been acting different lately.
HPI: He is able to answer questions, but appears to have trouble focusing. His wife reports that he has been more confused lately and has had mood changes. His wife reports his headache and other issues started after he fell at home about a month ago. He did not seek medical treatment after his fall. The patient’s wife reports he was bruised on his arms and head after the fall. Since his fall, the patient reports his headache has increased in intensity, but it is not unbearable. He also reports he has been dizzy and lightheaded lately. The patient reports he has been having problems with his memory over the past few weeks. He reports decreased visual acuity. He denies any muscle weakness. He also denies neck stiffness or paresthesias. He denies any photophobia or phonophobia. He denies any changes in bowel or bladder habits.
PMH: Illnesses — HTN, HLD, COPD; Medications — Lisinopril 5mg qd, Simvastatin 40mg qd, Albuterol inhaler prn, Budesonide inhaler bid
FMH: Mother passed away at age 75 of lung cancer; Father passed away at age 72 of MI; reports extensive family history of diabetes and hyperlipidemia
SH: Tobacco — 60 pack year history
ROS: Per HPI
PE:
General: Male patient appearance consistent with age. Patient is cooperative, but has trouble focusing during interview.
Vital Signs: BP:130/80, P:70, RR:18, BMI:30, T:100.9
HEENT: Normocephalic, atraumatic, PEERLA bilaterally. EOM intact bilaterally. No nuchal rigidity. Negative Brudzinski’s and Kernig’s signs.
Funduscopic: Optic disc visual bilaterally. Papilledema present bilaterally. No A/V nicking present.
Respiratory: Normal respirations present, no accessory muscle use. Normal, vesicular breath sounds present bilaterally. No wheezes, rales, or rhonchi present.
Musculoskeletal: Full ROM of extremities. No weakness noted in upper or lower extremities.
Psychiatric: Cooperative. Alert and orientated x 3. Appropriate mood and affect. No signs of response to visual or auditory hallucinations.
Neurologic: Cranial nerves II – XII grossly intact bilaterally. Muscle strength 5/5 in the upper and lower extremities bilaterally. DTRs are 2/4 in the upper and lower extremities bilaterally.
Tests –
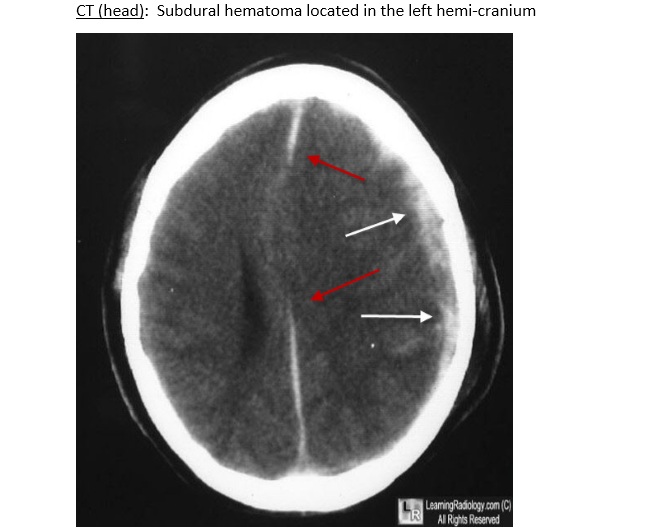
CT (head) – see below