Given these changes from the original case, what is your diagnosis?
What is your diagnostic explanation?
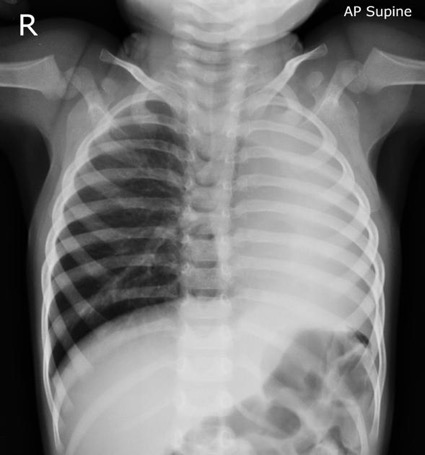
As compared to the long case, this patient is a 4 year old boy brought to the ED by his mother due to the sudden onset of coughing.
HPI: The boy’s mother states the cough began a few hours ago, along with wheezing. The child had been playing in his room alone prior to the onset of the cough. He has no history of asthma. She denies any episodes of apneas, fevers, lethargy, stridor, vomiting, or cyanosis. He has been eating normally the past few days. He has not had any sick contacts or prior occurrences.
FMH and SH are noncontributory.
ROS –
General: No lethargy, no change in appetite
HEENT: No episodes of otitis media, no nasal congestion/runny nose
Cardiovascular: Doesn’t complain of chest hurting or feeling his heart beat fast
Respiratory: See HPI
GI: No diarrhea/constipation, nausea/vomiting
GU: No problems with urination
Derm: No rashes
Neurology: No lethargy, listlessness
Heme: No bruising
PE –
VS: Temp 98.6, HR 106, BP 100/60, RR 30, Height 101cm (50th percentile), Weight 16kg (50th percentile)
General: Alert. No acute distress.
HEENT: Normocephalic, PERRLA, normal tympanic membranes, nose and oropharynx normal
Neck: No masses/lumps
Cardiac: RRR. Normal S1 and S2. No murmurs.
Lungs: Wheezing and diminished breath sounds on the right side on auscultation.
Abdomen: Bowel sounds present. No abdominal tenderness. No hepatomegaly. No abdominal distension.
Neuro: Good tone in all four extremities.
Skin: normal