Given these changes from the original case, what is your diagnosis?
What is your diagnostic explanation?
As compared to the long case, this patient is a 22 year old, previously healthy female presenting to the Emergency Department with diffuse chest discomfort that developed gradually over the past hour.
HPI: The patient states that her discomfort is a squeezing ache that does not radiate, change with position, or increase with palpation. Over the course of the past hour the discomfort has waxed and waned in intensity. Patient does not report diaphoresis, nausea, vomiting, dyspnea, palpitations, dizziness, or syncope. She states that last week she had a really bad cold consisting of rhinorrhea, congestion, fever, myalgia, and muscle tenderness, but this has nearly resolved. Patient reports no significant life stressors, no history of anxiety, no history of asthma, no correlation with meals, and no drug or alcohol use.
PE:
VS- BMI 21, HR 150, BP 126/84, RR 16, T 99.5 F
HEENT- WNL
Cardiovascular- Regular rate and rhythm, S1 and S2 are of normal intensity, S3 presents, no S4, no murmurs, T2 bilateral peripheral edema, pulses are 2+/4 bilaterally throughout, no bruits, no friction rub. Pain is not reproduced with palpation of chest. Elevated JVD (14 cm H2O)
Respiratory- Clear to auscultation in all lung fields bilaterally, no wheezing, or rales
Abdominal- Bowel sounds present in all four quadrants, nontender to light and deep palpation, liver edge is smooth and normal span, spleen is not palpable
Tests:
CXR – see below
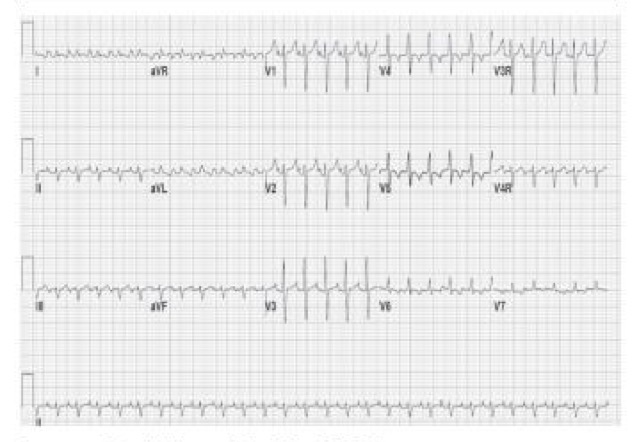
EKG – see below