Given these changes from the original case, what is your diagnosis?
What is your diagnostic explanation?
As compared to the long case, this patient is a 43 y/o female who presents to urgent care saying: “I woke up this morning with a fever and a really bad cough.” She clearly appears sick on general appearance and is in moderate distress.
HPI: Ms. Seaton notes that she awoke this morning feeling feverish, lethargic, and having a deep, painful cough. Cough is productive for 1-2 tablespoons of thick, yellow sputum. She denies experiencing any hemoptysis. Nothing seems to make the cough better or worse. Ms. Seaton says that she was “feeling achy” last night, but otherwise was not experiencing symptoms at that time. She reports feeling mildly short of breath and experiences mild pleuritic discomfort on her right side. Her temperature this morning when she awoke was 100.4. She states that a couple of her co-workers have been out of the office for similar symptoms this week.
PMH: Allergic to Penicillin, results in hives
SH: No current or prior tobacco use, drinks 1-2 glasses of wine once a month or for “special occasions”. Works as an electrical engineer at a local firm
FMH: Non-contributory
ROS: All pertinent history in HPI. Rest non-contributory
PE:
VS – Height 5’4’’, Weight 130lbs, BMI 22.3, HR 80, BP 136/88, RR 20, Temperature 101.2, Sa02- 93% on room air
HEENT – Normocephalic, atraumatic, PERRLA, pharynx shows moist, pink mucosa with no erythema or exudate
Cardiac – Normal S1, S2 present with no rubs, gallops, or murmurs.
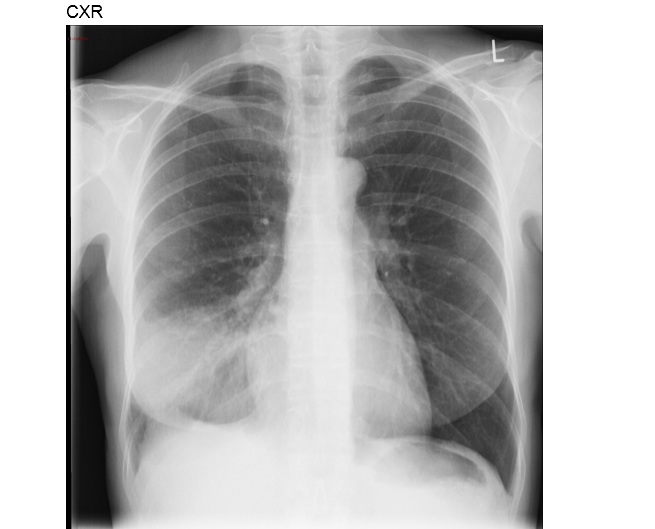
Lungs – Dullness to percussion at right lower lung base with resonance in all other lung fields. Auscultation reveals inspiratory crackles at right lower lung field with bronchial breath sounds. Auscultation of all other lung fields contain vesicular breath sounds with no adventitious sounds present.
Tests:
CBC –
Hemoglobin 13.0 mg/dl
Hct- 39%
RBCs- 4.9 million/mcl
WBCs- 15.2 million/mcl
Neutrophils- 88%”
CXR – see below
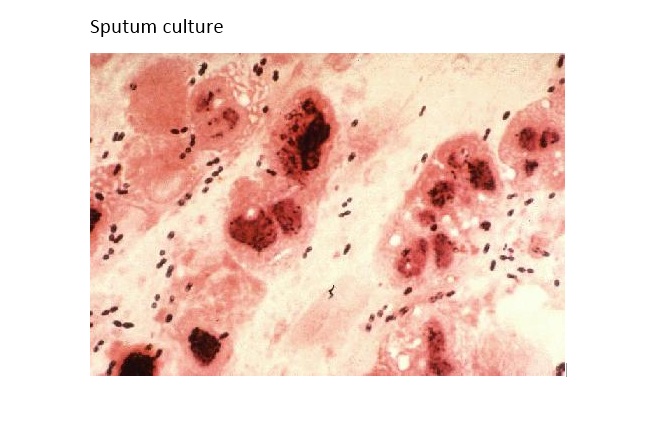
Sputum culture – see below